
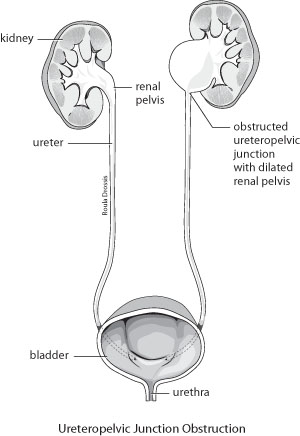
Percutaneous endopyelotomy is an effective treatment for patients with ureteropelvic junction obstruction. Ureteropelvic junction (UPJ) obstruction is a blockage in the area that connects the renal pelvis (part of the kidney) to one of the tubes (ureters) that move urine to the bladder. Obstruction of Percutaneous endopyelotomythe ureteropelvic junction (UPJ) can be caused by congenital abnormalities like fibrous scarring due to kidney stone or an earlier surgical procedure, a blood vessel which may kink the UPJ or an impacted stone in the upper part of ureter. This could lead to kidney tissue damage, formation of stones, infection, high blood pressure, deterioration of kidney function and eventually kidney failure. Endopyelotomy is a popular procedure to relieve all these symptoms. With percutaneous endopyelotomy, patients can expect up to a 90% success rate with little morbidity and minor disability.
UPJ obstruction generally occurs when a baby is still growing in the womb. This is called a congenital condition (present from birth). Most of the time, the blockage is caused when the connection between the ureter and the renal pelvis narrows. This causes urine to build up, damaging the kidney.
The condition can also be caused when a blood vessel is located in the wrong position over the ureter. In older children and adults, UPJ obstruction can be due to scar tissue, infection, previous treatments for a blockage or kidney stones.
UPJ obstruction is the most frequently diagnosed cause of urinary obstruction in children. It is now commonly diagnosed during prenatal ultrasound studies. In some cases, the condition isn't seen until after birth. Children may have an abdominal mass or a urinary tract infection
The most severe cases of UPJ obstruction may require surgery early in life. However, the majority of cases may not require surgery until later in life and some cases do not require surgery at all.
Symptoms
There may not be any symptoms. When symptoms occur, they may include:
Exams and Tests
Maternal pregnancy ultrasound may show kidney problems in the unborn baby.
Tests after birth may include:
Treatment
Surgery to correct the blockage lets urine to flow normally. Open (invasive) surgery is usually performed in infants. Adults may be treated with less-invasive procedures. These procedures involve much smaller surgical cuts than open surgery, and may include:
Recently, laparoscopy has been used to treat UPJ obstruction in children and adults who have not had success with other procedures.
A tube called a stent may be placed to drain urine from the kidney until the patient heals. A nephrostomy tube, which is placed in the patient's side to drain urine, may also be needed for a short time after the surgery. This type of tube may also used to treat severe infections before surgery.
Outlook (Prognosis)
Early diagnosis and treatment of UPJ obstruction may help preserve future kidney function. UPJ obstruction diagnosed before birth or early after birth may actually improve on its own.
Most patients do well with no long-term consequences. Significant kidney damage may occur in those who are diagnosed later in life. Current treatment options provide good long-term outcomes. Pyeloplasty provides the greatest long-term success.
In severe cases, rapidly taking pressure off the kidney (kidney decompression) immediately following birth may greatly improve kidney function.
Possible Complications
Permanent loss of kidney function (kidney failure) is a possible complication of untreated UPJ obstruction. Even after treatment, the affected kidney may be at increased risk for infection or kidney stones.
Percutaneous Access
Percutaneous endopyelotomy is completed with the patient in the prone position. In order to reduce the risk of infections, intravenous antibiotics are administered. Percutaneous access to the renal pelvis is completed optimally through an upper pole or middle pole calyx to help in the visualization of the UPJ. A wire is placed in antegrade fashion under fluoroscopic guidance across the UPJ obstruction, down the ureter, and into the bladder. In cases where antegrade guidewire placement is difficult, a guidewire can initially be placed in retrograde fashion. The guidewire, placed in retrograde fashion, is then finally exchanged for a percutaneous wire after dilation of the percutaneous tract. Placement of a guidewire across the UPJ obstruction is of critical importance since direct endoscopic vision of the renal pelvis is often unreliable to identify a pinpoint UPJ that not uncommonly is in an aberrant position. The percutaneous tract is dilated for nephroscopic examination of the renal pelvis and inspection of the UPJ obstruction. Blood clots if present are removed. If any stones are present, they are removed prior to incision of the UPJ obstruction. If the guidewire was placed initially in retrograde fashion, this wire is grasped with the forceps and pulled through the nephroscope sheath.
Endopyelotomy
The endopyelotomy knife is passed over the working wire and is seen under direct vision through the percutaneous nephroscope. Before proceeding with the incision the UPJ is balloon-dilated so the knife can easily be passed through the UPJ. Gentle dilation of the UPJ in this situation is critical so that ultimately the knife cuts the UPJ smoothly rather than pushing the UPJ away. Placement of the endopyelotomy knife is then completed to allow incision of the UPJ in the due-lateral position. The lateral position is determined by orienting the knife to the lateral position of the patient’s flank while referencing the position of the kidney on the excretory urogram or CT scan. The orientation of the cut is relatively easy to complete. However, in situations where the kidney is malrotated the orientation of the cut can be more challenging. The cut should also be made cautiously in patients that have previously undergone a failed UPJ repair. In this situation the vascular supply of the kidney relative to the UPJ may have changed.
After proper orientation, the knife is engaged under direct vision along the curve of the guidewire to allow a smooth, clean cut. By performing the incision under direct vision, the operator can identify the exact location and depth of the cut. In addition, extrapelvic structures such as aberrant vessels, often visualized by pulsation, can be identified and avoided. If significant bleeding is encountered at the time of the incision, allowing clot to form in the renal pelvis with subsequent vascular tamponade, typically controls hemorrhage. If arterial bleeding were to persist despite these measures, embolization may be required. The nephroscope enters the kidney through the upper pole and the UPJ is easily visualized. The knife will incise the UPJ obstruction laterally under direct vision. As the knife cuts the UPJ, the curve of the wire is followed and typically the wire is straightened in the process.
The other Urology Procedures are:
Few Major Hospitals for Endopyelotomy are:
Thailand, Malaysia, Singapore, Turkey and India are the most cost effective locations that offer up to almost 80% savings in comparison to the US.
SurgeryPlanet facilitates a plethora of services to the medical treatment traveler also which includes, a hassle free and discounted travel option, a welcome hand at the airport on arrival, travel in an air-conditioned car, round the clock service & support. Your medical evaluation is pre arranged with the least of waiting time. Once your assessment is complete and found medically fit, the procedure is immediately scheduled without a waiting period. Please read through our Services and Testimonials to understand and select your best options.
Major Treatments Abroad: Obesity / Bariatric Surgery | Spine Surgery | Stem Cell therapy | Fertility treatment | Knee replacement in India and Thailand | Heart Surgery | Organ transplant | Ayurveda Treatment | Heart valve replacement | Hip resurfacing | Hospitals in India and Thailand for Laparoscopic Sterilization| Best hospitals in Asia | JCI & ISO certified Hospitals | Cost effective medical procedures | Healthcare tourism | Complete privacy for affordable cost | Weight loss procedures | Infertility treatment | Board certified physicians | Low cost surgeries
SurgeryPlanet is an Healthcare Facilitator and not a Medical service provider. The information provided in this website is not to be used for diagnosis or treatment of any medical condition or use for any medical purposes. We provide information solely for medical travel facilitation and do not endorse any particular health care provider, hospital, facility, destination or any healthcare service or treatment listed. We are not an agent for, or affiliated to any health care provider, or service listed in our website and is not responsible for health care services provided by them. Choice of hospital or doctor for your healthcare services is your independent decision. Consult your domestic licensed health care provider before seeking the services of any health care provider you learn about from our website.

